Moxifloxacin hydrochloride.
Each film-coated tablet contains 436.8 mg of Moxifloxacin HCl equivalent to 400 mg of Moxifloxacin.
ATC Code: J01MA 14.
Pharmacology: Pharmacodynamics: Mechanism of action: Moxifloxacin is a 8-methoxy-fluoroquinolone antibiotic with a broad spectrum of activity and bactericidal action. Moxifloxacin has in vitro activity against a wide range of Gram-positive and Gram-negative organisms, anaerobes, acid-fast bacteria, and atypicals e.g. Chlamydia spp., Mycoplasma spp., and Legionella spp.
The bactericidal action results from the interference with topoisomerase II and IV. Topoisomerases are essential enzymes which control DNA topology and assist in DNA replication, repair and transcription. Moxifloxacin exhibits concentration dependent bactericidal killing. Minimum bactericidal concentrations are generally similar to minimum inhibitory concentrations.
Moxifloxacin is effective against b-lactam and macrolide resistant bacteria. Studies in animal models of infection have demonstrated high in vivo activity.
Resistance: Resistance mechanisms which inactive penicillins, cephalosporins, aminoglycosides, macrolides and tetracyclines do not interfere with the antibacterial activity of moxifloxacin. There is no cross resistance between moxifloxacin and these agents. Plasmid-mediated resistance has not been observed to date.
It appears that the C8-methoxy moiety contributes to enhanced activity and lower selection of resistant mutants of Gram-positive bacteria compared to the C8-H moiety. The presence of the bulky bicycloamine substituent at the C-7 position prevents active efflux, a mechanism of fluoroquinolone resistance.
In vitro studies have demonstrated that resistance to Moxifloxacin develops slowly by multiple step mutations.
A very low overall frequency of resistance was demonstrated (10-7 – 10-10). Serial exposure of organisms to sub-MIC concentrations of moxifloxacin showed only a small increase in MIC values.
Cross resistance among quinolones has been observed. However, some gram-positive and anaerobic organisms resistant to other quinolones are susceptible to moxifloxacin.
Effects on the intestinal flora in humans: In a study, the changes in the intestinal flora were seen following oral dosing with moxifloxacin. E. coli, Bacillus spp., Bacteroides vulgatus, Enterococci, and Klebsiella spp. were reduced, as were the anaerobes Bifidobacterium, Eubacterium, and Peptostreptococcus. These changes returned to normal within two weeks. Clostridium difficile toxin was not found.
Pharmacokinetics: Absorption and bioavailability: Following oral administration moxifloxacin is absorbed rapidly and almost completely. The absolute bioavailability amounts to approx. 91%.
Pharmacokinetics are linear in the range of 50 – 1200 mg single dose and up to 600 mg once daily dosing over 10 days. Steady state is reached within 3 days. Following a 400 mg oral dose peak concentrations of 3.1 mg/L are reached within 0.5 – 4 h p.a. Peak and trough plasma concentrations at steady state (400 mg once daily) were 3.2 and 0.6 mg/L, respectively.
Concomitant administration of moxifloxacin together with food slightly prolongs the time to reach peak concentrations by approximately 2 hours and slightly reduced peak concentrations by approximately 16%. Extent of absorption remained unchanged. As AUC/MIC is most predictive for antimicrobial efficacy of quinolones, this effect is clinically not relevant. Therefore, moxifloxacin can be administered independent from meals.
After a single 400 mg intravenous 1 h infusion peak concentrations of approximately 4.1 mg/L were reached in the plasma at the end of infusion which corresponds to a mean increase of approx. 26% relative to the oral application. Exposure to drug in terms of AUC at a value of approximately 39 mg*h/L is only slightly higher compared to the exposure after oral administration (35 mg*h/L) in accordance with the absolute bioavailability of approximately 91%.
Following multiple intravenous dosing (1h infusion), peak and trough plasma concentrations at steady state (400 mg once daily) were between 4.1 to 5.9 and 0.43 to 0.84 mg/L respectively. At steady-state the exposure to drug within the dosing interval is approximately 30% higher than after the first dose. In patients mean steady state concentrations of 4.4 mg/L were observed at the end of a 1h infusion.
Distribution: Moxifloxacin is distributed very rapidly to extravascular spaces. Exposure to drug in terms of AUC (AUCnorm = 6 kg*h/L) is high with a volume of distribution at steady state (Vss) of approx. 2 L/kg. in saliva peak concentrations higher than those of plasma may be reached. In in vitro and ex vivo experiments over a range of 0.02 to 2 mg/L a protein binding of approximately 45% independent from the concentration of the drug was determined. Moxifloxacin is mainly bound to serum albumin. Due to this low value high free peak concentrations > 10 x MIC are observed.
Moxifloxacin reaches high concentrations in tissues like lung (epithelial fluid, alveolar macrophages, biotic tissue), the sinuses (maxillary and ethmoid sinus, nasal polypi) and inflamed lesions (cantharide blister fluid) where total concentrations exceeding those of the plasma concentrations are reached. High free drug concentrations are measured in interstitial body water (saliva, intramuscular, subcutaneous). In addition, high drug concentrations were detected in abdominal tissues and fluids and female genital tract.
The peak concentrations and site vs. plasma concentration ratios for various target tissues yielded comparable results for both modes of drug administration after a single dose of 400 mg moxifloxacin.
Metabolism: Moxifloxacin undergoes Phase II transformation and is excreted via renal and biliary/faecal pathways as unchanged drug as well as in form of a sulfo-compound (M1) and a glucuronide (M2). M1 and M2 are the only metabolites relevant in humans, both are microbiologically inactive. Neither in in vitro nor in clinical Phase I studies metabolic pharmacokinetic interactions with other drugs undergoing Phase I biotransformation involving Cytochrome P-450 enzymes were observed.
Independent from the route of administration the metabolites M1 and M2 are found in the plasma at concentrations lower than the parent drug. Preclinical investigations adequately covered both metabolites thus excluding potential implications with respect to safety and tolerability.
Elimination: Moxifloxacin is eliminated from plasma with a mean terminal half life of approximately 12 hours. The mean apparent total body clearance following a 400 mg dose ranges from 179 to 246 ml/min. Renal clearance amounted to about 24 - 53 ml/min suggesting partial tubular reabsorption of the drug from the kidneys. Concomitant administration of ranitidine and probenecid did not alter renal clearance of the drug.
Mass balance of the mother compound and Phase II metabolites of moxifloxacin yielded an almost complete recovery of approx. 96 - 98% independent from the route of administration with no indication of oxidative metabolism.
Elderly: Pharmacokinetics of moxifloxacin are not affected by age.
Gender: There was a 33 % difference in the pharmacokinetics (AUC, Cmax) of moxifloxacin between male and female subjects. Drug absorption was unaffected by gender. These differences in the AUC and Cmax were attributable to the differences in body weight rather than gender. They are not considered as clinically relevant.
Interethnic difference: Possible interethnic differences were examined in Caucasian, Japanese, Black and other ethnic groups. No clinically relevant interethnic differences in pharmacokinetics could be detected.
Paediatric: Pharmacokinetics of moxifloxacin were not studied in paediatric patients.
Renal impairment: The pharmacokinetics of moxifloxacin are not significantly changed by renal impairment (including creatinine clearance < 30 ml/min/1.73m2) and in patients on chronic dialysis i.e. hemodialysis and continuous ambulatory peritoneal dialysis.
Liver impairment: Moxifloxacin plasma concentrations of patients with mild to severe hepatic impairment (Child Pugh A to C) did not reveal clinically relevant differences compared to healthy volunteers or patients with normal hepatic function, respectively.
Toxicology: Preclinical safety data: In a local tolerability study performed in dogs, no signs of local intolerability were seen when moxifloxacin was administered intravenously. After intraarterial injection inflammatory changes involving the peri-arterial soft tissue were observed suggesting that intra-arterial administration of moxifloxacin should be avoided.
Carcinogenicity, Mutagenicity: Although conventional long-term studies to determine the carcinogenic potential of moxifloxacin have not been performed, the drug has been subject to a range of in vitro and in vivo genotoxicity tests. In addition, an accelerated bioassay for human carcinogenesis (initiation/promotion assay) was performed in rats. Negative results were obtained in 4 strains of the Ames test, in the HPRT mutation assay in Chinese harmster ovary cells and in the UDS assay in rat primary hepatocytes. As with other quinolones the Ames test with TA 102 was positive and the in vitro test in the Chinese harmster v79 cells showed chromosomal abnormalities at high concentrations (300 mcg/mL). However, the in vivo micronucleus assay in the mouse was negative. An additional in vivo assay, the dominant lethal assay in the mouse, was negative as well. It is concluded that the negative in vivo results adequately reflect the in vivo situation in terms of genotoxicity. No evidence of carcinogenicity was found in an initiation/promotion assay in rats.
ECG: At high concentrations, moxifloxacin is an inhibitor of the delayed rectifier potassium current of the heart and may thus cause prolongations of the QT-interval. Toxicological studies performed in dogs using oral doses of ≥ 90 mg/kg leading to plasma concentrations ≥ 16 mg/L caused QT-prolongations, but no arrhythmias. Only after very high cumulative intravenous administration of more than 50 fold the human dose (>300 mg/kg), loading to plasma concentrations of ≥ 200 mg/L (more than 30 fold the therapeutic level after intravenous administration), reversible, non-fatal ventricular arrhythmias were seen.
Arthrotoxicity: Quinolones are known to cause lesions in the cartilage of the major diarthodial joints in immature animals. The lowest oral dose of moxifloxacin causing joint toxicity in juvenile dogs was four times maximum recommended therapeutic dose (400 mg/50 kg person) on mg/kg basis, with plasma concentrations two to three times higher than those at the recommended therapeutic dose.
Reprotoxicity: Reproductive studies performed in rats, rabbits and monkeys indicate that placental transfer of moxifloxacin occurs. Studies in rats (per os and i.v.) and monkeys (per os) did not show evidence of teratogenicity or impairment of fertility following administration of moxifloxacin. Skeletal malformations were observed in rabbits that had been treated with an intravenous dose of 20 mg/kg. This study result is consistent with the known effects of quinolones on skeletal development. There was an increase in the incidence of abortions in monkeys and rabbits at human therapeutic concentrations. In rats, decreased foetal weights, an increased prenatal loss, a slightly increased duration of pregnancy and an increased spontaneous activity of some male and female offspring was observed at doses which were 63 times the maximum recommended dose on a mg/kg basis with plasma concentrations in the range of the human therapeutic dose.
Moxifloxacin Hydrochloride tablets are indicated for the treatment of adults (≥ 18 years of age) with the following bacterial infections caused by susceptible strains: Acute sinusitis,
Acute exacerbations of chronic bronchitis,
Community acquired pneumonia,
Mild to moderately severe inflammatory pelvic diseases (i.e. infections of the upper female genital tract, including salpingitis and endometritis), without an associated tubo-ovarian or pelvic abscess.
Moxifloxacin Hydrochloride tablets are not recommended for monotherapy of mild to moderately severe inflammatory pelvic diseases. Preferably, they should be administered in combination with another suited antibiotic (such as cephalosporin), due to the increasing resistance of Neisseria gonorrhoeae to moxifloxacin; that is, unless moxifloxacin-resistant Neisseria gonorrhoeae can be ruled out.
Complicated skin and skin structure infections,
Complicated intra-abdominal infections including polymicrobial infections such as abscesses.
Adults: One 400 mg film-coated tablet once daily.
Mode of administration: Oral route of administration.
Only limited data on overdose are available. Single doses of up to 1200 mg and multiple doses of 600 mg moxifloxacin over 10 days were administered to healthy subjects without any significant undesirable effects. In the event of overdosage it is recommended that appropriate supportive care including ECG measurements should be instituted as dictated by the patient's clinical status.
The use of charcoal early after oral administration may be useful to prevent excessive increase of systemic exposure to moxifloxacin in cases of overdosage.
Known hypersensitivity to any component of Moxifloxacin or other quinolones or any of the excipients.
Pregnancy and lactation.
Patients below 18 years of age.
In some instances, the hypersensitivity and allergic reactions already occurred after the first administration and the doctor should be informed immediately.
Anaphylactic reactions in very rare instances can progress to a life threatening shock, in some instances after the first administration. In these cases the treatment with moxifloxacin has to be discontinued, medical treatment (e.g. treatment for shock) is required.
Moxifloxacin has been shown to prolong the QT interval on the electrocardiogram in some patients. As women tend to have a longer baseline QTc interval compared with men, they may be more sensitive to QTc-prolonging medications. Elderly patients may also be more susceptible to drug-associated effects on the QT interval.
As the magnitude of QT prolongation may increase with increasing concentrations of the drug, the recommended dose and the infusion rate (400 mg within 60 minutes) should not be exceeded. However, in patients suffering from pneumonia no correlation between plasma concentrations of moxifloxacin and QTc prolongation was observed. QT prolongation may lead to an increased risk for ventricular arrhythmias including torsades de pointes. No cardiovascular morbidity or mortality attributable to QTc prolongation occurred with moxifloxacin treatment in clinical studies with more than 9000 patients, however certain predisposing conditions may increase the risk for ventricular arrhythmias.
Therefore, treatment with moxifloxacin should be avoided due to the lack of clinical experience with the drug in these patient populations: In patients with known prolongation of QT interval,
In patients with uncorrected hypokalemia,
In patients receiving class IA (e.g. quinidine, procainamide) or class III (e.g. amiodarone, sotalol) antiarrhythmic agents.
Moxifloxacin should be used with caution as an additive effect of moxifloxacin on the QT interval cannot be excluded for the following conditions: In patients treated concomitantly with drugs that prolong the QT interval such as cisapride, erythromycin, antipsychotics and tricyclic antidepressants.
In patients with ongoing proarrhythmic conditions, such as clinically significant bradycardia, acute myocardial ischemia.
In patients with liver cirrhosis as preexisting QT prolongation in these patients cannot be excluded.
In women and elderly patients who, both, may be more susceptible to QTc-prolonging drugs.
Cases of fulminant hepatitis potentially leading to liver failure (including fatal cases) have been reported with moxifloxacin. Patients should be advised to contact their doctor immediately prior to continuing treatment if symptoms related to liver failure occur.
Cases of bullous skin reactions like Stevens-Johnson syndrome or toxic epidermal necrolysis have been reported with moxifloxacin. Patients should be advised to contact their doctor immediately prior to continuing treatment if skin and/or mucosal reactions occur.
Seizures may occur with quinolone therapy. It should be used with caution in patients with known or suspected CNS disorders which may predispose to seizures or lower the seizure threshold. Antibiotic associated colitis has been reported with the use of broad-spectrum antibiotics including moxifloxacin; therefore it is important to consider this diagnosis in patients who develop serious diarrhea in association with the use of moxifloxacin. In this clinical situation adequate therapeutic measures should be initiated immediately. Drugs inhibiting peristalsis are contraindicated in patients who develop serious diarrhea.
Moxifloxacin should be used with caution in patients with myasthenia gravis because the symptoms can be exacerbated.
The risk of developing fluoroquinolone-associated tendonitis and tendon rupture is further increased in people older than 60, in those taking corticosteroid drugs, and in kidney, heart, and lung transplant recipients. Patients experiencing pain, swelling, inflammation of a tendon or tendon rupture should be advised to stop taking their fluoroquinolone medication (moxifloxacin) and to contact their health care professional promptly about changing their antimicrobial therapy. Patients should also avoid exercise and using the affected area at the first sign of tendon pain, swelling, or inflammation.
For patients with complicated pelvic inflammatory disease (e.g. associated with a tuboovarian or pelvic abscess), for whom an intravenous treatment is considered necessary, treatment with Moxifloxacin 400 mg film-coated tablets is not recommended.
In patients for whom sodium intake is of medical concern (patients with congestive heart failure, renal failure, nephrotic syndrome, etc.) the additional sodium load of the solution for infusion should be taken into account.
Pregnancy: The safe use of moxifloxacin in human pregnancy has not been established. Reversible joint injuries are described in children receiving some quinolones, however this effect has not been reported as occurring on exposed fetuses. Animal studies have shown reproductive toxicity. The potential risk for humans is unknown. Consequently, the use of moxifloxacin during pregnancy is contraindicated.
Lactation: As with other quinolones, moxifloxacin has been shown to cause lesions in the cartilage of the weight bearing joints of immature animals. Preclinical evidence indicates that small amounts of moxifloxacin may be secreted in human milk. There is no data available in lactating or nursing women. Therefore, the use of moxifloxacin in nursing mothers is contraindicated.
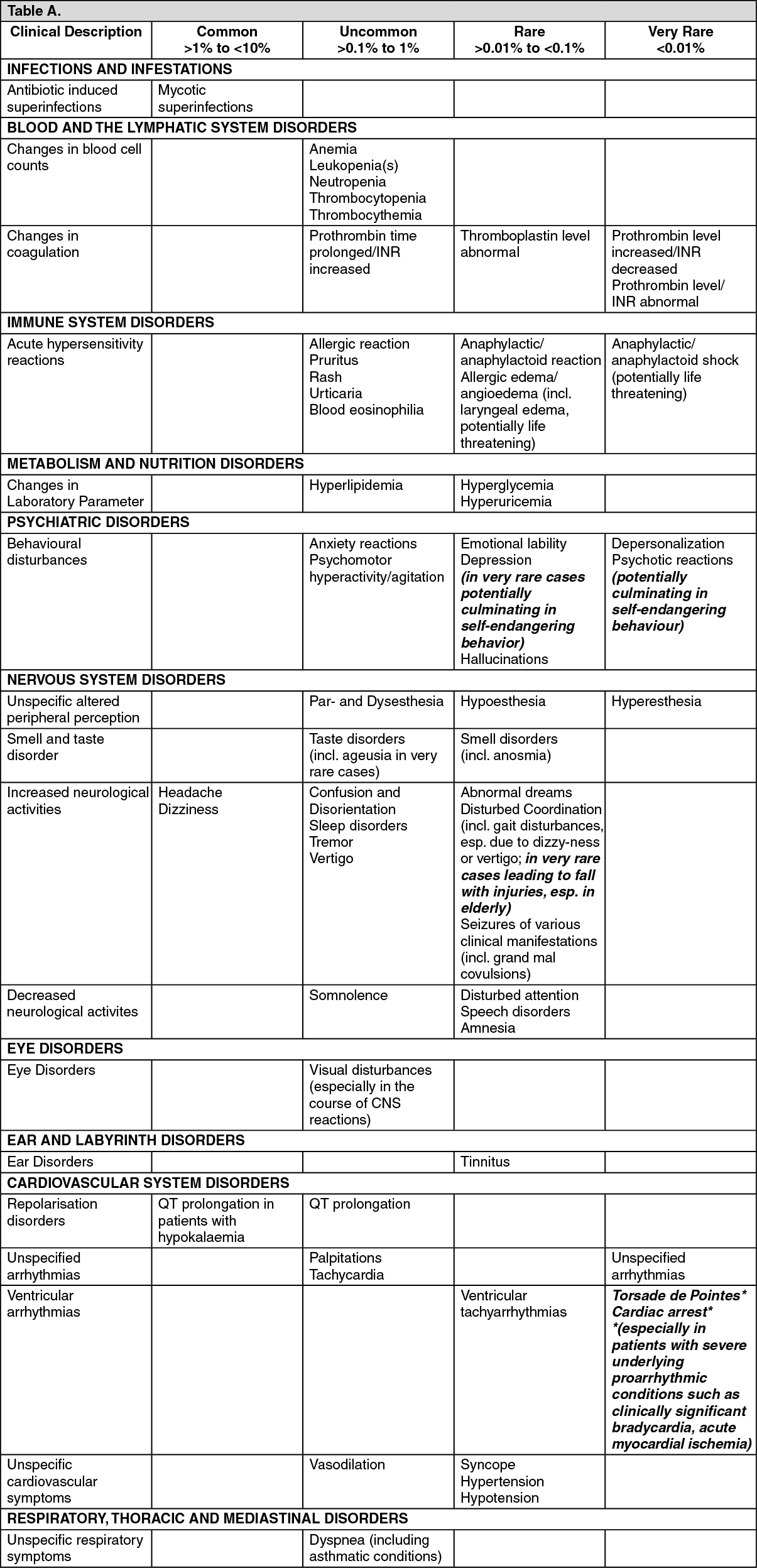
(See tables.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Common:
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Common: Increased gamma-glutamyl-transferase.
Uncommon: Ventricular tachyarrhythmias, Hypotension, Oedema, Antibiotic associated colitis (in very rare cases associated with life threatening complications), Seizures of various clinical manifestations (incl. grand mal convulsions), Hallucinations, Renal impairment and Renal failure (due to dehydration esp. in elderly with pre-existing renal disorders).
Antacids, minerals and multi-vitamins: Concomitant ingestion of moxifloxacin together with antacids, minerals and multi-vitamins may result in impaired absorption of moxifloxacin after oral administration due to formation of chelate complexes with the multi-valent cations contained in these preparations. This may lead to plasma concentrations considerably lower than desired. Hence, antacids, antiretroviral drugs (e.g. didanosine), and other preparations containing magnesium or aluminium, sucralfate and agents containing iron or zinc should be administered at least 4 hours before or 2 hours after ingestion of an oral moxifloxacin dose.
Warfarin: No interaction during concomitant treatment with warfarin on pharmacokinetics, prothrombin time and other coagulation parameters has been observed.
Changes in INR (International Normalized Ratio): Cases of increased anticoagulant activity have been reported in patients receiving anticoagulants concurrently with antibiotics, including moxifloxacin. The infectious disease (and its accompanying inflammatory process), age and general status of the patient are risk factors. Although an interaction between moxifloxacin and warfarin was not demonstrated in clinical trials, INR monitoring should be performed and, if necessary, the oral anticoagulant dosage should be adjusted as appropriate.
Digoxin: The pharmacokinetics of digoxin are not significantly influenced by moxifloxacin and vice versa. After repeated dosing in healthy volunteers moxifloxacin increased Cmax of digoxin by approximately 30% at steady state without affecting AUC or trough levels.
Charcoal: Concomitant dosing of charcoal and 400 mg oral moxifloxacin reduced the systemic availability of the drug by more than 80% by preventing absorption in vivo. The application of activated charcoal in the early absorption phase prevents further increase of systemic exposure in cases of overdose.
After intravenous drug administration carbo medicinalis only slightly reduces systemic exposure (approx. 20%).
Food and dairy products: Absorption of Moxifloxacin was not altered by food intake (including dairy products). Moxifloxacin can be taken independent from food intake.
Store below 30°C and protect from moisture.
Shelf-Life: 24 months.
J01MA14 - moxifloxacin ; Belongs to the class of fluoroquinolones. Used in the systemic treatment of infections.
Moxi 400 FC tab 400 mg
10 × 10's


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image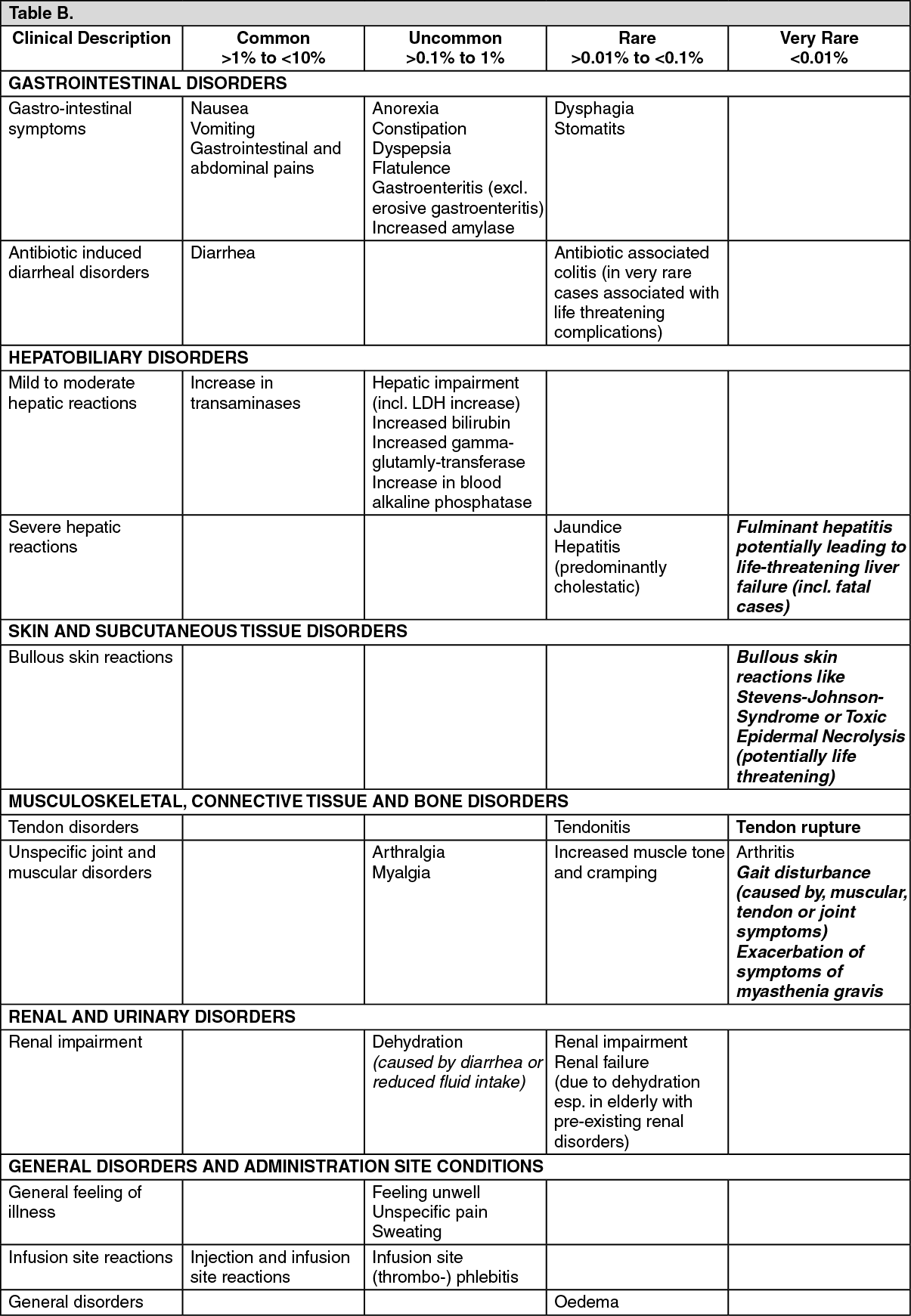 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out
